

Quebec’s specialist doctors need to bring their union back down to earth
Sometimes, too much is as bas as too little.

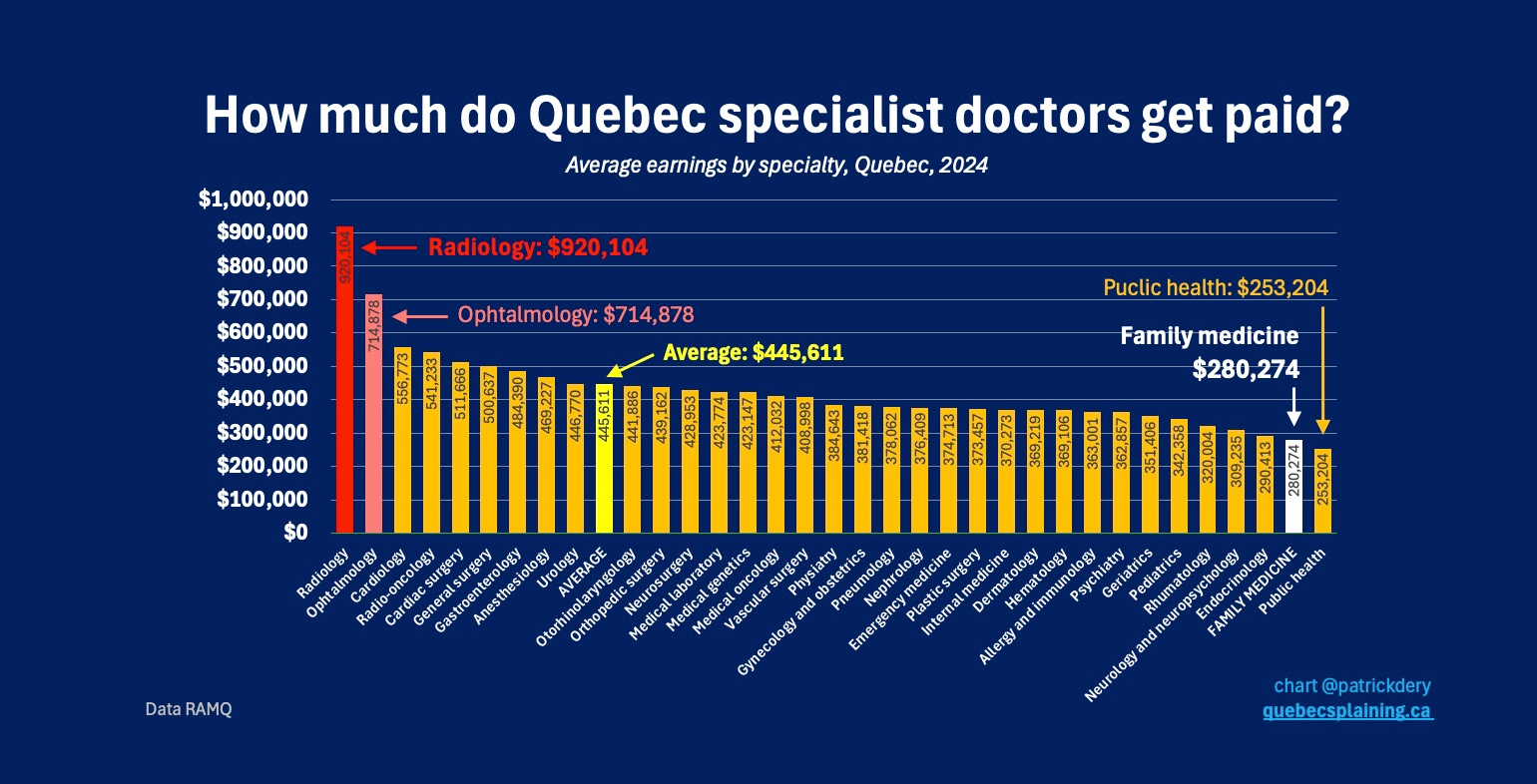
The Fédération des médecins spécialistes du Québec (FMSQ) is angry.
Negotiations with the government have reached a deadlock. The FMSQ is now boycotting the system through which consultation requests …
